CastlePreferences
Content
Add NewCastle Preferences:
Read “Rules of the house of God”
Lasix dose= Age + BUN
Operating after radiation: 1 week for every 10 gy they receive.
Every robot case he wants:
Baby laps
2 purple clip appliers, RARPS get the Gold Clip Applier
Blunt trocars
Vessel sealer
Local preference: 0.25% marcaine AND 1% lidocaine with epi
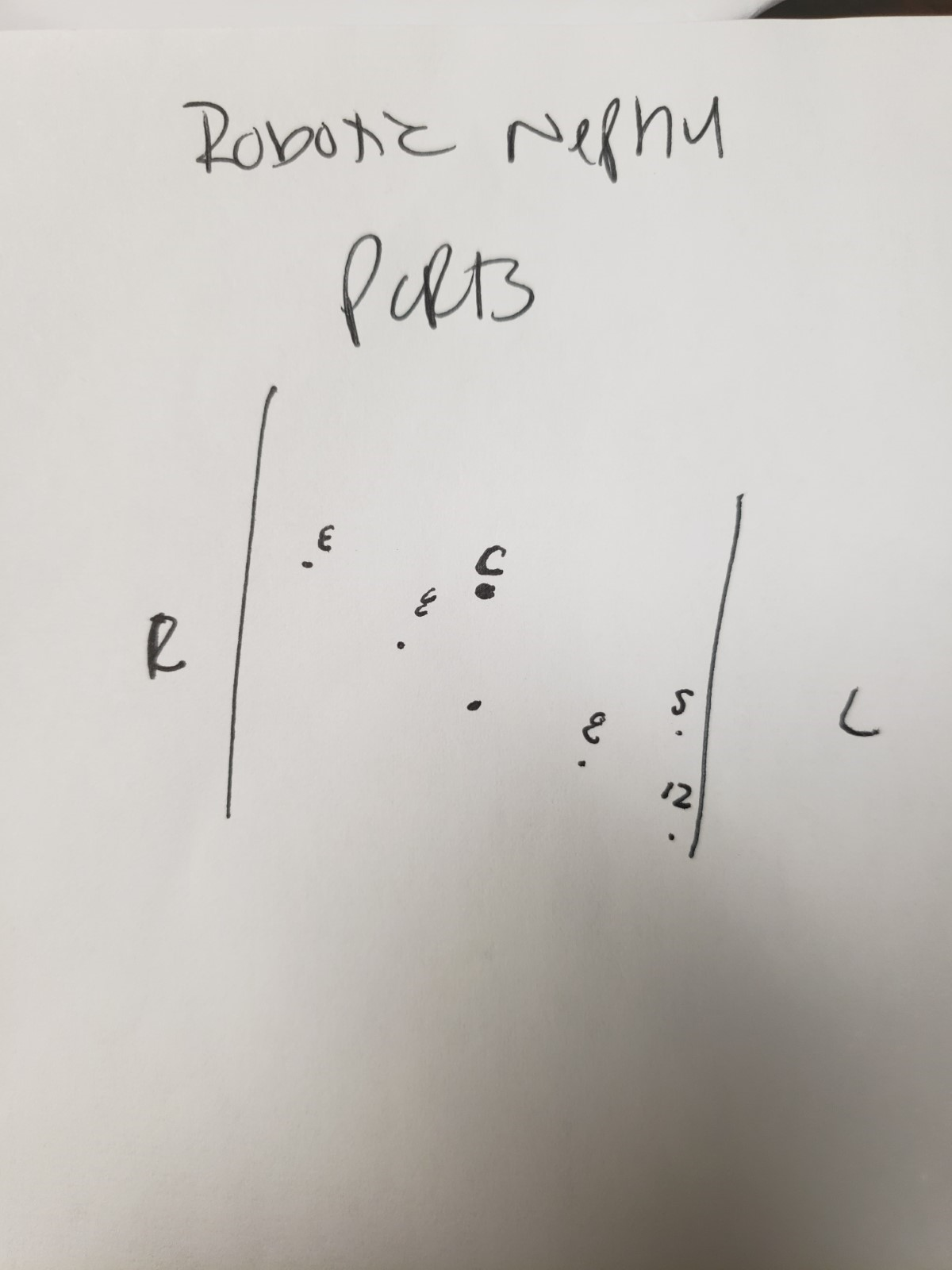
Always 2 working assistant ports (so on a right kidney you need a 12 and 2 5 mm ports one for liver and one to work with)
After ALL MAJOR CASES get a post op H&H and BMP
For kidney cases mark the patient’s midline in preop!
Kidney case positioning:

Use large yellow gel roll which goes under the mattress.
Tape at chest, hip, above knees, and above ankles. For chest and hip wrap around bed and use a full roll
Nephroureterectomy:
positioning: Same as kidney, but prep in genitals. So in male you tape below the scrotum rather than at the hip. Foley is placed on the field.
Does not want airseal due to risk of cancer seeding. Uses 15 assistant port.
needles 3-0 V lock CV23 6 in x2; 3-0 V lock V20 6 in
Ports: Camera midline 4 fingers above umbilicus
IVC thrombectomy needs:
-5-0 prolene C1 6 inches x4
-3-0 prolene SH 6 inches x 4
-Gortex suture 4-0 x4
-Bull dogs with silk ties
-4 vessel loops
-Stapler; lap and robotic available
-airseal
-20 cm bag
-heparinized saline 100,000 units heparin per 1L saline
-Position like nephrectomy, make sure to mark midline and go around the umbilicus
Partial nephrectomy:
MAG3 prior to surgery and post-surgery
Always starts off clamp but puts bulldogs in near the hilum.
Likes to do US early on in the case
Sutures:
4-0 monocryl RB1 dyed (if possible) 6 inches no clips x 2
3-0 monocryl SH clip, lapraty, knot 6 inches x3
2-0 vicryl SH clip, lapraty, knot 8 inches x4
0 vicryl CT1 clip, lapraty, knot 6 inches x2
5-0 prolene 6 inches in case of bleeding from vessels
Silk sutures on bulldogs
5 mm laparoscopic debaky clamp
Fascia for 12 port 0 vicryl on UR6 and 1 vicryl on CT1 x2 for extraction site
For dictation when US used wants a separate part of findings called: “Ultrasound findings and professional interpretation”
Post op care: If he leaves a drain for concern for urine leak, he will want the foley to come out and then get JP Cr 4-5 hours after catheter is removed.
Follow up:
-3 week post op visit (this is because most pseudoaneurysms would present by then) with BMP and Hgb
-3 month H&H, BMP, CTU, MAG3
-Then follow up based on the pathology
-Oncocytoma treats like T1a and gets CTU and labs at 9 months
Nephrectomy:
On left always takes the lumbar
100 solumedrol in OR
50 solumedrol q12 post op
25 solumedrol q8h POD 1-2
Prostatectomy:
-4-0 Monocryl dyed RB1: uses for bleeding
-3-0 Vlock CV23 9 inch x 2 and 6 inch x1 (uses 1 9 in for DVC suture and usually a 9 and 6 as double armed for anastomosis but depending on size of BN may sometimes use 2 9 inches)
-Anastomosis starts at 5 o'clock and then runs. Uses pully system to tighten.
-Almost always does BN recon: 2 layers 6 in CV23 3-0 vlock and 4-0 monocryl
-18 fr final foley
-No type and screen needed
-Lymph nodes: 2
Starts case with LN dissection
Standardly does external iliac, obturator, and internal iliac
Boundaries: Distal= circumflex iliac vein; lateral = genitofemoral nerve; medial= ureter and obliterated umbilical artery; proximal is essentially where the ureter crosses the iliacs.
Opens up peritoneum lateral to medial umbilical ligament, carries this down toward vas. Transects vas and clips both sides. Continues opening peritoneum to the ureter. Then defines the boundaries of the LND. Finds obliterated umbilical, opens up space all the way down to endopelvic fascia and sometimes opens that. Starts with external. Marches anterior to external iliac artery. Clips proximally and distally. Then develops space of Marseille (lateral to the iliac vessels). Finds the nerve and once the nerve is found vessel seals proximally and then along the nerve distally. Always goes parallel to the nerve. Then flips to the medial side of vessels and clips distally.
Runs DVC with 9 in CV23 vlock then goes back to middle and through pubic bone
Takes the DVC then oversews with a Vlock (Runs all the way across and then back to middle and then trhru the bone) and then takes the urethra. Does this so he knows he isn’t getting the urethra in his sutures.
Follow up:
7-10 days for foley removal. Likes to have abx started the day before the catheter removal.
3 months with PSA prior
CYSTECTOMY:
If previously radiated then he likes to bowel prep with enema before. Mag citrate bottle the day before and an enema the night before and then an enema in preop.
If Hgb less than 11 on preop labs typically likes to preadmit and give blood before surgery.
Mark ostomy site in preop!!! Make sure to have them sit and stand. Needs to overly rectus muscle.
Movantik 25 mg PO in preop
Every Cystectomy have 1g Meropenem as preop abx
For female cystectomy does not extract specimen through the vagina due to risk of seeding the vaginal cuff with cancer.
Wound Ostomy Nurse:
Nicole Kalbacher: 601-320-7330 or 504-988-3721
Does not use air seal for any urothelial cases
For case:
15 and 12 mm assistant ports (non airseal)
Handheld Ligasure (likes the impact)
Nylon suture for drain stitch
19 fr blake drain
5 blue loads for GIA 75 mm stapler OR 4 loads of GIA 100
Red rubber catheter
Ureteral diversion stents
4-0 dyed monocryl RB1 x6
4-0 chromic SH x2
3-0 silk pops 2 packs
3-0 Vicryl SH x4
4-0 vircyl RB1 x 4
3-0 vicryl SH 6 inches
Vlock 9 in V20 for DVC stitch
Balfour or Alexis
18 fr foley for pelvic drain
Nu Knit
Gel foam
Gold clips with vicryl tied to them one dyed and one undyed
Gerald’s with teeth
Frasier tip or pediatric tip suction
POST OP:
If CO2<21 wants bicarb 650 mg PO once or twice a day
Discharge home on lovenox 40 mg subq daily for 30 days
He wants the patients to drink 60 oz of Gatorade or diabetic of equivalent EVERY DAY at home.
He wants them to have a protein shake with every meal.
Need and H&H and CMP ordered for follow up and lab slip needs to be handed to them before they leave.
6 week loop-o-gram to make sure there is no stricture of the anastomoses.
3 month follow up:
CBC, CMP, CXR, CT urogram, PSA (if applicable), B12 (yearly), cytology (yearly)
T2 disease get follow up every 6 months for 2 years then yearly with above labs/imaging
T3 disease get follow up every 6 months for 3 years then yearly with above labs/imaging
Neobladders:
Foley stays for 3 weeks and gets a cystogram before removal.
CT Urogram at 6 weeks post op to make sure anastomoses are open.
Transplant reimplant:
Position supine, split leg on pink pad like a prostate. Can leave one arm out if needed. Surgery will be done in about 20-30 degree Trendelenberg. Assistant will be on the opposite side of the kidney. Can dock robot from right or between the legs
Ports: similar to prostate, a little higher, and aimed a bit toward the side that the kidney is on.
Dyed 4-0 monocryl for ureterovesical anastomosis
3-0 v-lock on CV23 x2 for first layer of bladder-just mucosa and a little detrusor
3-0 v-lock on V20 x2 for second layer of bladder –likes to get good detrusor bite and mucosa
4-0 monocryl to suture stent in place
6 fr x 12 cm JJ ureteral stent (in transplant cart)
Opens bladder horizontally. Implants ureter into the posterior flap of bladder a 1-2 cm from the edge. Closes bladder vertically.
Stent stays for 4-6 weeks.
Prostate biopsies:
Prefers Cipro. No IM ABx in clinic.
Blocks the prostate in the trans view. Likes to inject into rectal wall. Goes sagittal to block the apex.
Takes 12 core if no MRI fusion. Doesn’t specify medial lateral.
Looks at both trans and sagittal before biopsy.
Miscellaneous info:
If patient is going to have indwelling foley he likes bacitracin to tip of penis
80 mg of gent into contrast for loopogram, nephrostogram
If you injure a vessel give 3000 units of heparin especially if it is an arterial injury
Staplers: number indicates open height of the staple itself
4.5 mm staple – colon
3.5 mm staple – small bowel
2.5 mm staple – vascular
2.0 mm staple – fine vascular
Afex male incontinence device: essentially a cup that the penis goes in that drains to a leg bag. About $80-90. Doesn’t work for small penises. Must be standing up.
Prompt PGS https://www.promptpgs.com/ cheek swab. Germline testing to assess baseline risk for prostate cancer
TULANE MAILING ADDRESS for discs:
1415 Tulane Ave
Box: HC15
Attn: Erik Castle, MD Urology
New Orleans, LA 70112